Restrictive Cardiomyopathy in Cats: Clinical Characteristics and Management
Restrictive cardiomyopathy (RCM) is a primary cardiac disease in cats characterized by myocardial stiffness and diastolic dysfunction (restrictive pathophysiology). It is the second most common cardiac disease in cats. In humans, RCM is typically divided into two main types: those primarily involving the endocardium (endocardial RCM) and those primarily involving the myocardium. This classification appears to also apply to cats, with the endocardial form referred to as myocardial fibrosis.
Myocardial RCM involves prominent fibrotic foci or diffuse involvement of the endocardium or myocardium, primarily affecting the left ventricle (LV), and to varying degrees causes left ventricular chamber distortion and/or obstruction. These diseases result in elevated left ventricular diastolic pressure, reduced left ventricular filling from normal to reduced (decreased compliance). Elevated diastolic pressure leads to left atrial enlargement, pulmonary venous stasis or pulmonary edema. Left ventricular contractility is generally normal or mildly impaired.
In humans, endocardial RCM can be caused by myocardial endocardial fibrosis (Loeffler endocarditis and tropical endocardial fibrosis) and endocardial elastic fiber proliferation (primary and secondary). The cause of feline myocardial RCM is not clear, but it is considered multifactorial, as clinical presentation and pathotype have a wide spectrum.
The feline specific diagnostic and morphological standards have not yet been established like in humans. To better understand the epidemiology and clinical features of feline endocardial RCM, 41 necropsy cases diagnosed between 2005 and 2014 were examined.

Clinical findings:
40 were domestic cats, 1 was a Persian cat. The average age at death was 7.3 years, ranging from 4 months to 19 years, with a standard deviation of 4.5 years. Sex distribution: 25 males (19 neutered), 16 females (13 spayed).
Of the 41 cats, 30 were due to respiratory distress, with 6 also having pareses of the hind limbs or due to aortic thromboembolic paresis (ATE). Another 11 cats only had hind limb paresis or paralysis. Common findings at initial physical examination included dyspnea (n=35), tachycardia (n=28), depressed heart sounds and lung sounds (n=24), absent femoral pulses (n=17), arrhythmias (n=12), abdominal distension (n=10), systolic heart murmurs (n=8), and heart racing (n=7). The thyroid was not palpable in any case.
CBCs and serum biochemical analyses were performed on 37 cats. CBCs results were within normal limits in 29 cats, The remaining 8 cats had mild leukocytosis (n=5) or mild anemia (n=3). Serum biochemical abnormalities included elevated urea nitrogen (n=13), transaminases and creatine kinase activity (n=14), and mild to marked elevation (n=2).
Chest radiographs were performed on 38 cats, which typically showed mild to moderate cardiac enlargement, with significant enlargement of the left atrium or left atrium and right atrium (n=36). Pleural effusion was present in 27 cases, and pulmonary edema in 19 cases. Abdominal radiographs confirmed ascites (n=12) and hepatomegaly (n=9).
Ultrasound examinations were performed on 34 cats. 19 cats had solitary or combined records of various arrhythmias, including atrial premature contractions (PACs; n=9), atrial fibrillation (AF; n=5), ventricular premature contractions (PVCs; n=5), right bundle branch block (RBBB; n=4), complete atrioventricular block (CAVB; n=1) and first-degree AV block (1AVB; n=1).
All 41 cats' echocardiograms typically showed severe left atrial enlargement (n=29) or biatrial enlargement (n=12), left ventricular hypertrophy and interventricular septal thickening. Irregular echoes were present in the left ventricular inner side (n=36). Endocardial thickening plaques were commonly found associated with the connection between LVFW and VS (n=25). Echocardiography revealed 8 cats with thrombus in the LA. Mild to moderate mitral and/or tricuspid regurgitation was consistently present on Doppler examination (n=38).
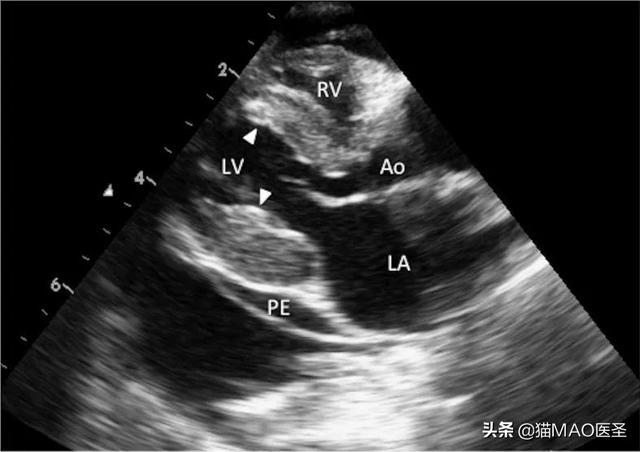
A 7-year-old female domestic shorthair cat's right-sided chest long-axis ultrasound view showed left atrial enlargement and an irregular high-echoed endocardial area (arrow). Ao, aorta; LA, left atrium; LV, left ventricle; PE, pericardial effusion; RV, right ventricle.
All 41 cats attempted treatment. The treatment regimen included diuretics, positive inotropic drugs, ACE inhibitors, and antiarrhythmic drugs. The results were generally poor, with half of the cats dying of severe left or biventricular congestive heart failure (CHF) or recurrent ATE within 1 month of clinical onset, with an average survival time of 30 days (range 1 to 977 days).
Summary
Of the 41 cats, except for one Persian cat, the others were domestic cats, with no obvious breed preference; this is consistent with previous reports. In a necropsy study of 25 cats, 22 were domestic cats and 3 were Siamese cats. In addition, cases have been reported in Burmese, Siamese, Persian and domestic short-haired and long-haired cats, but the specific breed preference has not been confirmed.
This group of 41 cases presented with left ventricular or biventricular CHF, including dyspnea, tachycardia, pleural effusion, ascites, pulmonary edema and ATE-related paresis of the hind limbs. 8 cats had systolic murmurs accompanied by mitral and/or tricuspid regurgitation and arrhythmias. CBCs were generally within normal limits and no significant pathological findings were detected. Serum biochemical results largely reflected the process of ATE onset. Chest radiographs typically showed varying degrees of cardiac enlargement, pleural effusion and pulmonary edema. Ultrasound showed left ventricular inner side endocardial thickening, left atrium or biatrial enlargement.
As with previous descriptions, these clinical findings were similar, including a high risk of ATE. Thrombus in the left ventricular inner side was not associated with the occurrence of hind limb paresis or paralysis. The incidence of PACs (26%; 9/34) and AF (15%; 5/34) was not unusual in the observations of 19 cats either solitary or combined with varying degrees of arrhythmias.
In the cases, the duration of the disease ranged from 1 day to 977 days, with an average survival time of 30 days, despite aggressive medical treatment. Prior reports, 16 cats had RCM, with 12 cats presenting with symptoms and the mean survival time was 21 days, and the other 1277 days; nearly half of the cats did not survive for more than 1 month. Therefore, the short survival time of affected cats, as confirmed in this study. In other words, most of the affected cats were diagnosed late, likely because symptoms may not be obvious before significant myocardial dyspnea progressed.
The results confirm and extend the findings of previous studies, and draw the following conclusions, despite the limitations of this study, including its small size and retrospective and necropsy-based nature.
First, feline myocardial RCM may be more common than previously thought, as high-endocardial fibrotic abnormalities may be missed on echocardiography.
Second, there is a male predominance (male/female ratio of 1.56), although it is difficult to strictly compare this ratio with the male cat population in previous necropsy populations.
Third, medical treatment for left or biventricular CHF is generally ineffective, although some cats have been able to treat pleural effusion and pulmonary edema for more than 1 year.
Finally, the prognosis of feline myocardial RCM is poor; many affected cats die of severe CHF or ATE, with an average survival time of 1 month.