Cat Clinical Manifests Hypokalemia, Possible Cause is Primary Aldosteronism - Immediate Differentiation Needed
I am @Dr. Mao the cat, follow me to share daily pet disease 'hardcore', welcome to leave a message and private message to exchange
Primary aldosteronism is a renal disease, characterized by excessive aldosterone secretion and independence.
Primary aldosteronism was first described in humans in 1955, and discussed three features: hypertension, hypokalemia, and elevated serum aldosterone concentration. Initially considered a rare disease, it has been found in about 11% of patients with arterial hypertension and in about 8% of patients with resistant hypertension.
The first case of primary aldosteronism in cats was reported in 1983. Despite being one of the most common adrenal cortical diseases in cats, it is not often diagnosed in veterinary practice. Many cases of arterial hypertension, hypokalemia, or both, can be attributed to chronic kidney disease (CKD) as the primary disease, but primary aldosteronism has been proven to be a cause and is associated with the progression of CKD.
Aldosterone is a glucocorticoid hormone with a strong mineralocorticoid activity, produced by the mineralocorticoid cells of the renal zonal band. Aldosterone production is driven and regulated by two mechanisms: 1) the renin-angiotensin-aldosterone system; and 2) by potassium direct regulation. The renin-angiotensin-aldosterone system is activated by decreased circulating blood volume and renal blood flow. This leads to reduced sodium and chloride transport into cells, including dense tubule of the distal limb, and renin secretion. Renin converts angiotensinogen (produced by the liver) into angiotensin I, which is hydrolyzed by angiotensin-converting enzyme (ACE) into angiotensin II. Angiotensin II stimulates aldosterone secretion.
When hypokalemia occurs, potassium ions directly depolarize the mineralocorticoid cells, independently of the renin-angiotensin-aldosterone system, to regulate aldosterone secretion. ACTH is also the third stimulant of aldosterone production. Studies have shown that administration of synthetic ACTH results in significant differences in plasma aldosterone concentration.
Circulating aldosterone targets renal, colonic, and salivary gland tissues, and binds to the cell membrane of these epithelial cells. The response to circulating aldosterone is sodium reabsorption in the distal limb of the nephron, which increases water retention, and potassium excretion in the urine. Because of the vasoconstrictor effect of angiotensin II, plasma and extracellular fluid volume increases with increased peripheral total resistance, leading to hypertension. Potassium is excreted in the urine, reducing plasma potassium concentration.
Cellular extracellular fluid volume increase leads to an increase in blood flow to the kidney, reducing renin secretion. Hypokalemia solves potassium release, which restores the potassium of the mineralocorticoid cell, these two mechanisms constitute the negative feedback loop of aldosterone secretion.
Excess aldosterone secretion can be due to primary or secondary causes.
Primary aldosteronism: It can be caused by adrenal tumor mass (adenoma or carcinoma, hatchery or primary), or by adrenal hyperplasia.
If suspected of primary aldosteronism, measure plasma aldosterone concentration and compare it with the concurrent plasma potassium concentration.Imaging examinations such as abdominal ultrasound, magnetic resonance imaging (MRI) and computed tomography can identify adrenal abnormalities and can assess to other abdominal organs and surrounding tissues for metastasis and tumor invasion.

In cats, primary aldosteronism has been increasingly recognized and diagnosed, but its prevalence may be underestimated.
II
CKDIIⅡCKD
IICKD
132.5 mEq/L=45.5 mEq/L148-168meq/L=140-160meq/L6837iu/L<120iu/L1312>170mmHg

PRAPACPRAPACPRA
4PRAPACPACPAC
ACTHACTH
ACTHcosyntropin25μg/cat2.5μg/kgcosyntropin125μg/cat1575cosyntropin
5μg/kg60-75PAC
PACPAC
MRICT
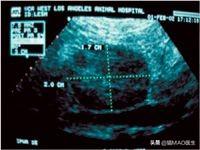
1.7×2
13.5cm
CKDCKD
T4





















